論文報告(六) · Paper VI
Global Patterns of Substance Use and Multi-Dimensional Outcomes among Incarcerated Youth: A Systematic Review
全球受監禁青少年物質使用與多維度結果:系統性回顧
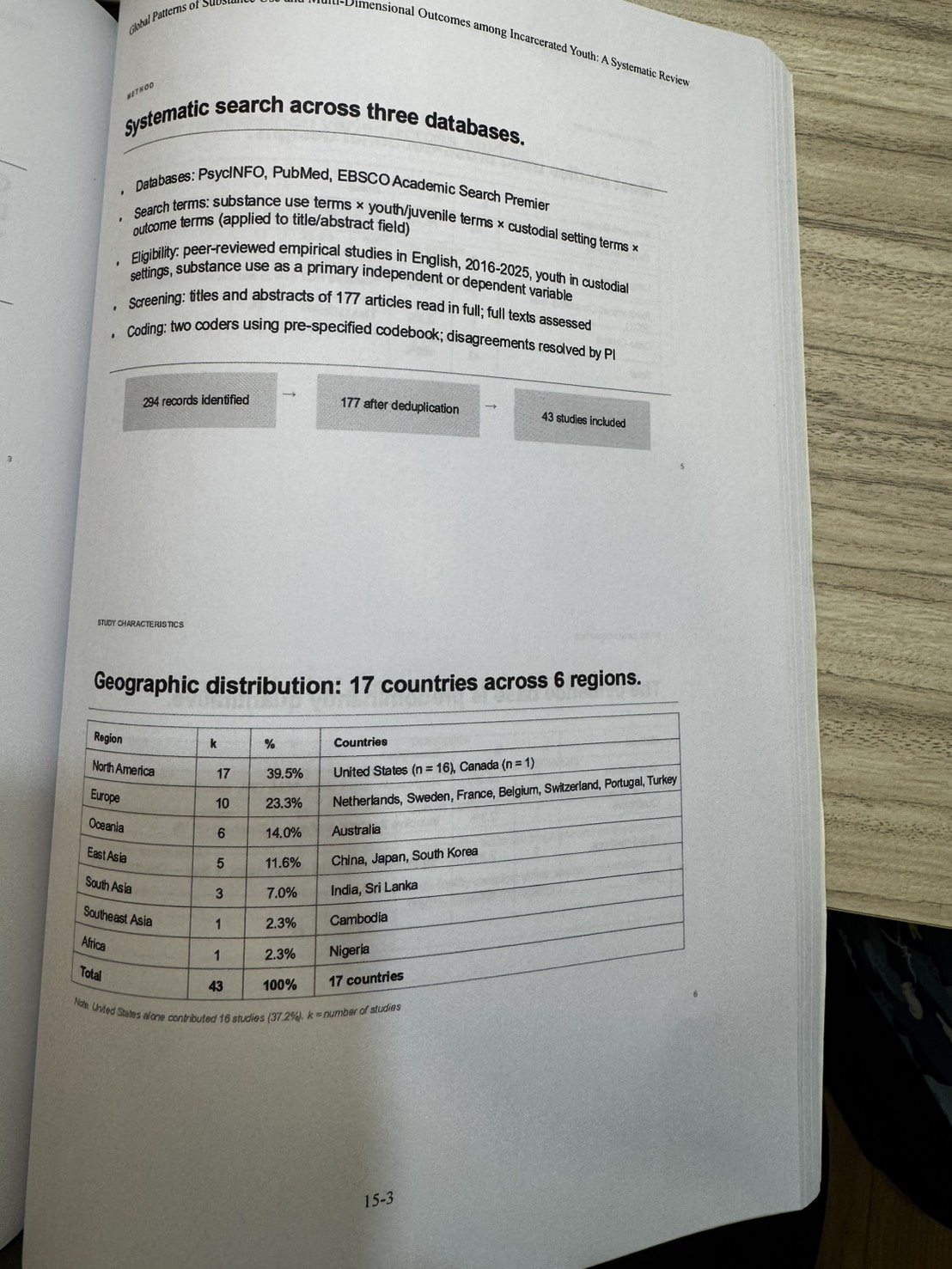
2016-2025 年 17 個國家、43 篇研究的系統性回顧。童年創傷是物質使用的主要前置因子(66.7%),而物質使用又預測再犯(40%)、精神共病(40%)、攻擊(24%)、自殺自傷(24%)——兩個並行卻互不對話的研究傳統,首次被本文整合於同一分析框架。
這場是下午論文場的方法學壓軸——Tzu-Ying Lo 教授(紐約聖約翰大學)以系統性回顧(PRISMA 規範)橫掃 2016-2025 年全球 43 篇受監禁青少年物質使用研究, 指出該領域 60 年來累積的結構性分裂:一支研究問「什麼導致用藥」、另一支研究問「用藥導致什麼」—— 兩股力量「互相不認識卻在回答同一個問題」。本研究是第一篇將兩個分析傳統整合於同一分析框架的回顧。
Core Thesis · 核心論述
- 物質使用不是一個離散的行為問題——而是童年逆境 × 精神共病 × 結構劣勢更廣網絡中的一個節點,同時是過去傷害的產物,也是後續傷害的驅動。
- 兩個並行研究傳統,互不對話:
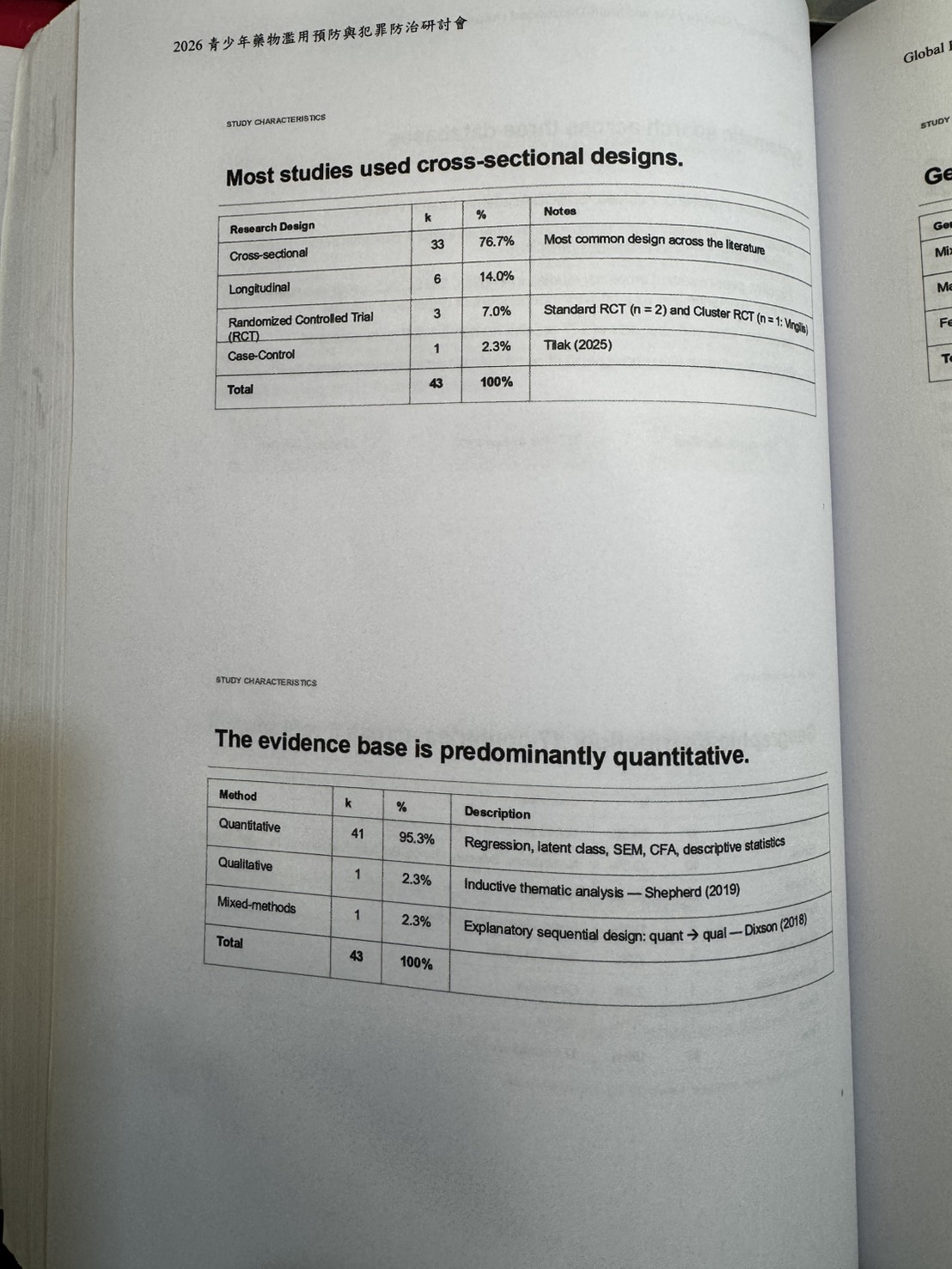
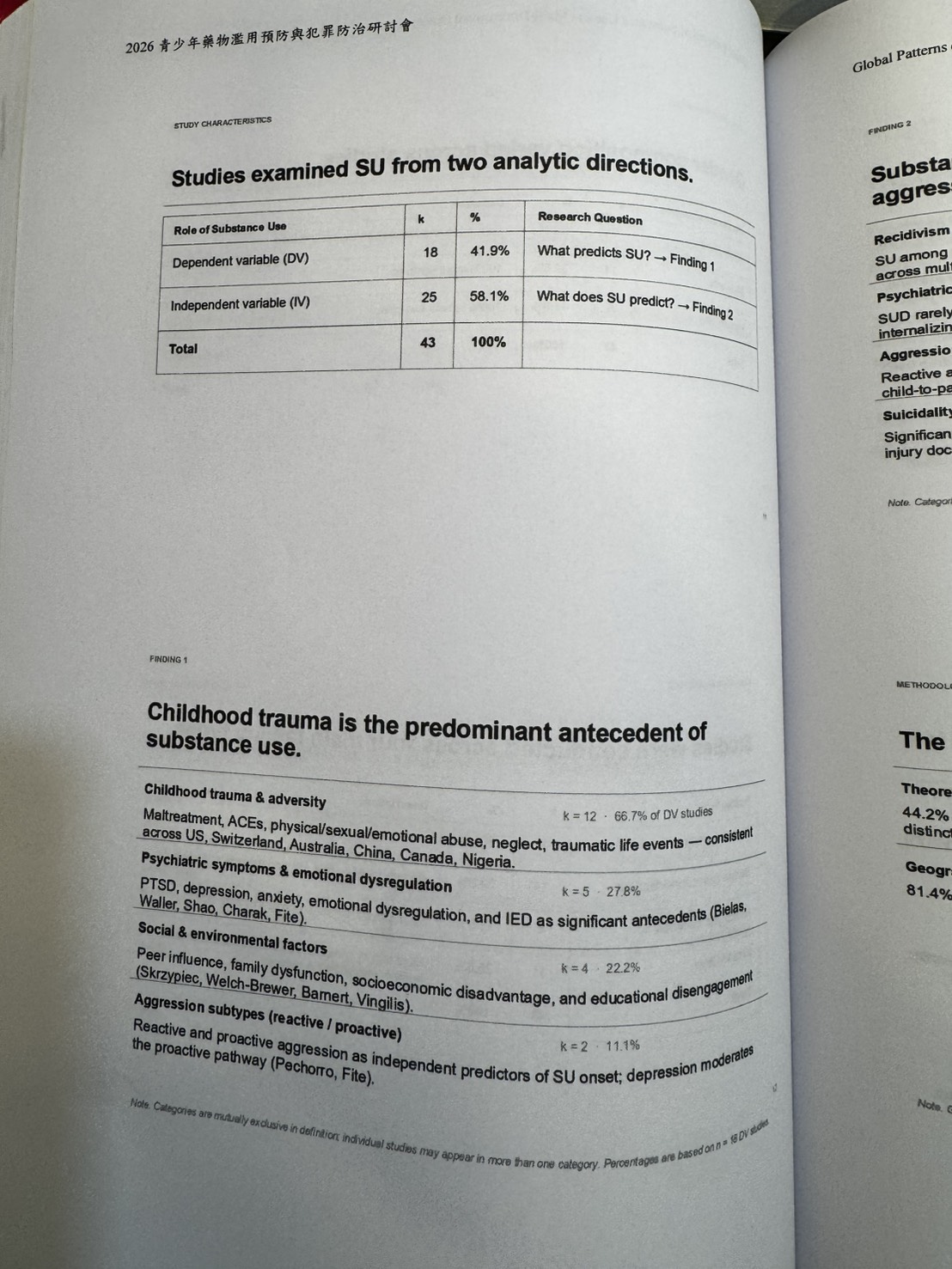
- (1) SU as antecedent(前置):18 篇(41.9%)——童年創傷、逆境、精神病理為主要前置因子。
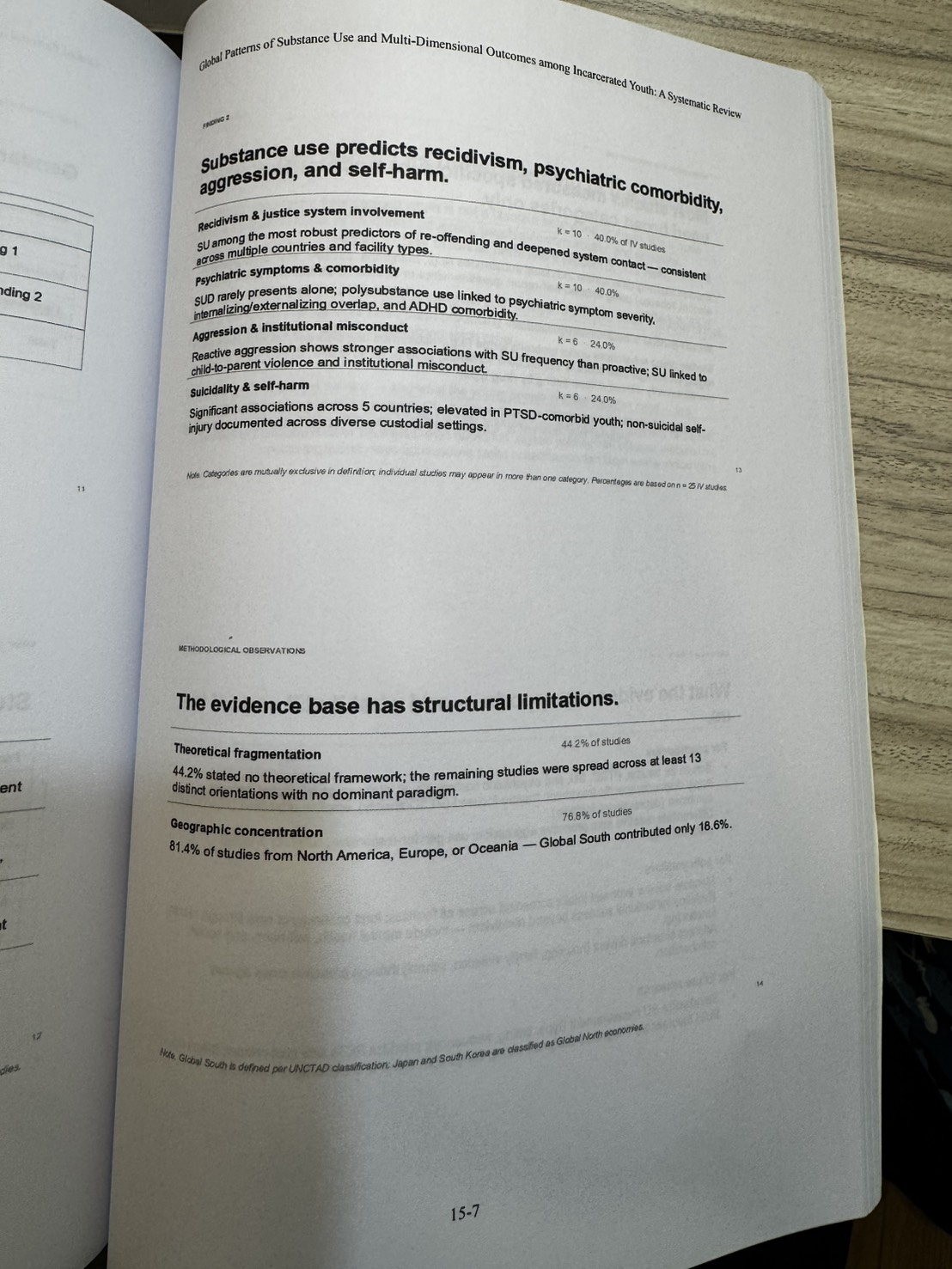
- (2) SU as consequence(後果):25 篇(58.1%)——預測再犯、攻擊、自殺、機構適應不良。
- 童年創傷是預測物質使用的最強單一因子(k=12, 66.7%)——maltreatment、ACEs、性/身/情緒虐待、忽視,跨美、瑞士、澳、中、加、奈及利亞一致。
- 「機構成功」應重新定義——不能只看「再犯」,更要看心理健康、自殺自傷、社會功能。
- 該領域的結構性限制:44.2% 研究無理論框架、81.4% 來自北美/歐洲/大洋洲——Global South 的聲音嚴重缺席。
論文內容重點 · Paper Walkthrough
本場關鍵數字 · Key Numbers
43 / 17 / 60% / 66.7% / 40% / 44.2% / 81.4%
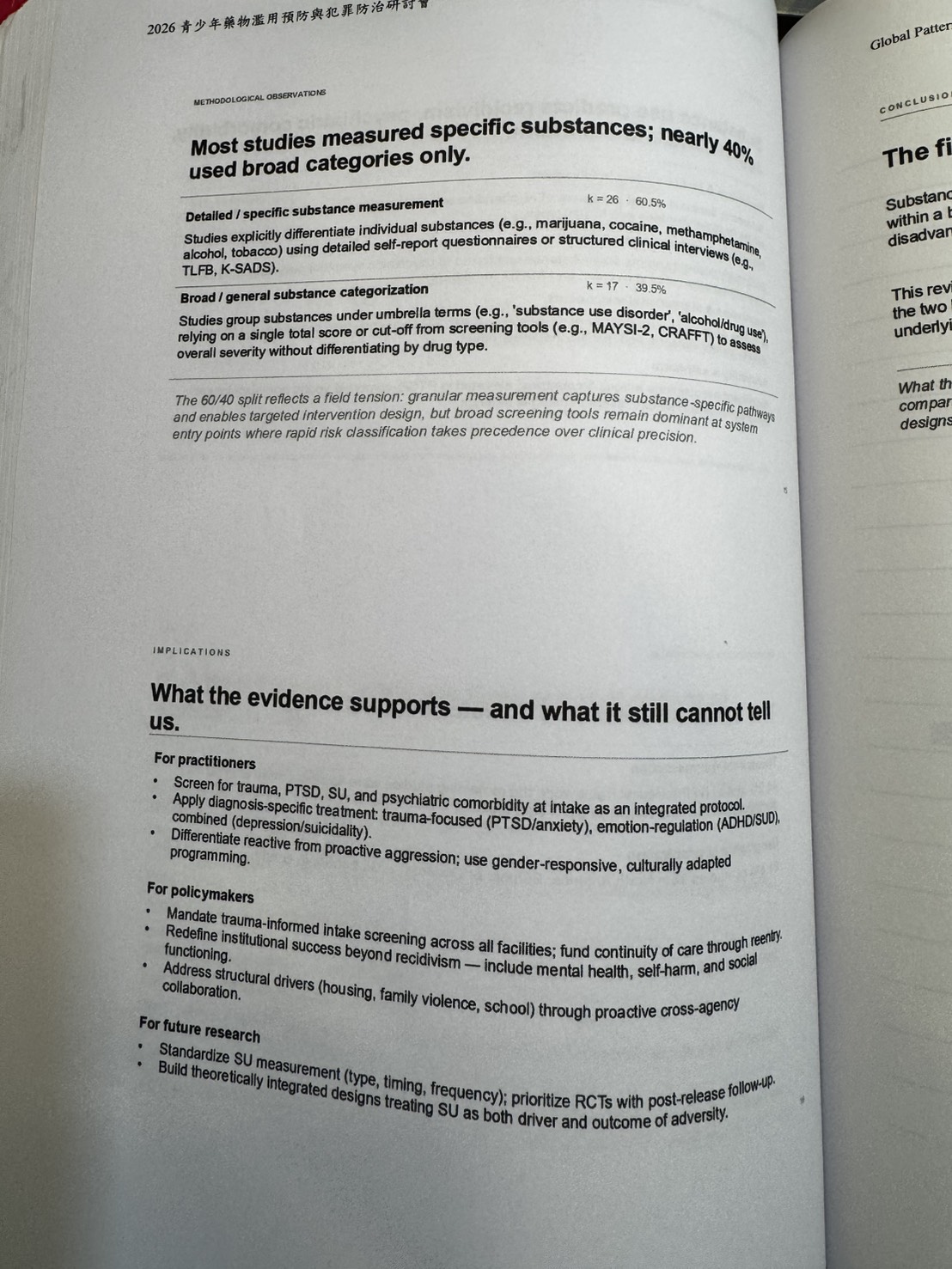
43=納入研究篇數;17=國家數;60%=美國受監禁青少年罹患 SUD 比例;
66.7%=童年創傷在前置因子研究中的佔比(最高);40%=SU 預測再犯/精神共病的研究佔比;
44.2%=無理論框架的研究比例;81.4%=研究來自北美/歐洲/大洋洲的集中度(Global South 嚴重失語)。
對台灣矯正政策的政策意涵
- 「機構成功」應重新定義——再犯不應是唯一指標,必須納入心理健康、自殺自傷、社會功能;呼應上午第 4 場白鎮福「全人復元」典範。
- Trauma-informed intake screening 應成為制度標配——所有矯正學校入校時應整合創傷/PTSD/SU/精神共病的篩查;可與第 1 場鄭元皓「再犯風險自動計算介面」整合。
- Diagnosis-specific treatment 需要本土化——trauma-focused、emotion-regulation、combined 三軌處遇方案,建議由矯正署、衛福部心健司、教育部學特司共同推動。
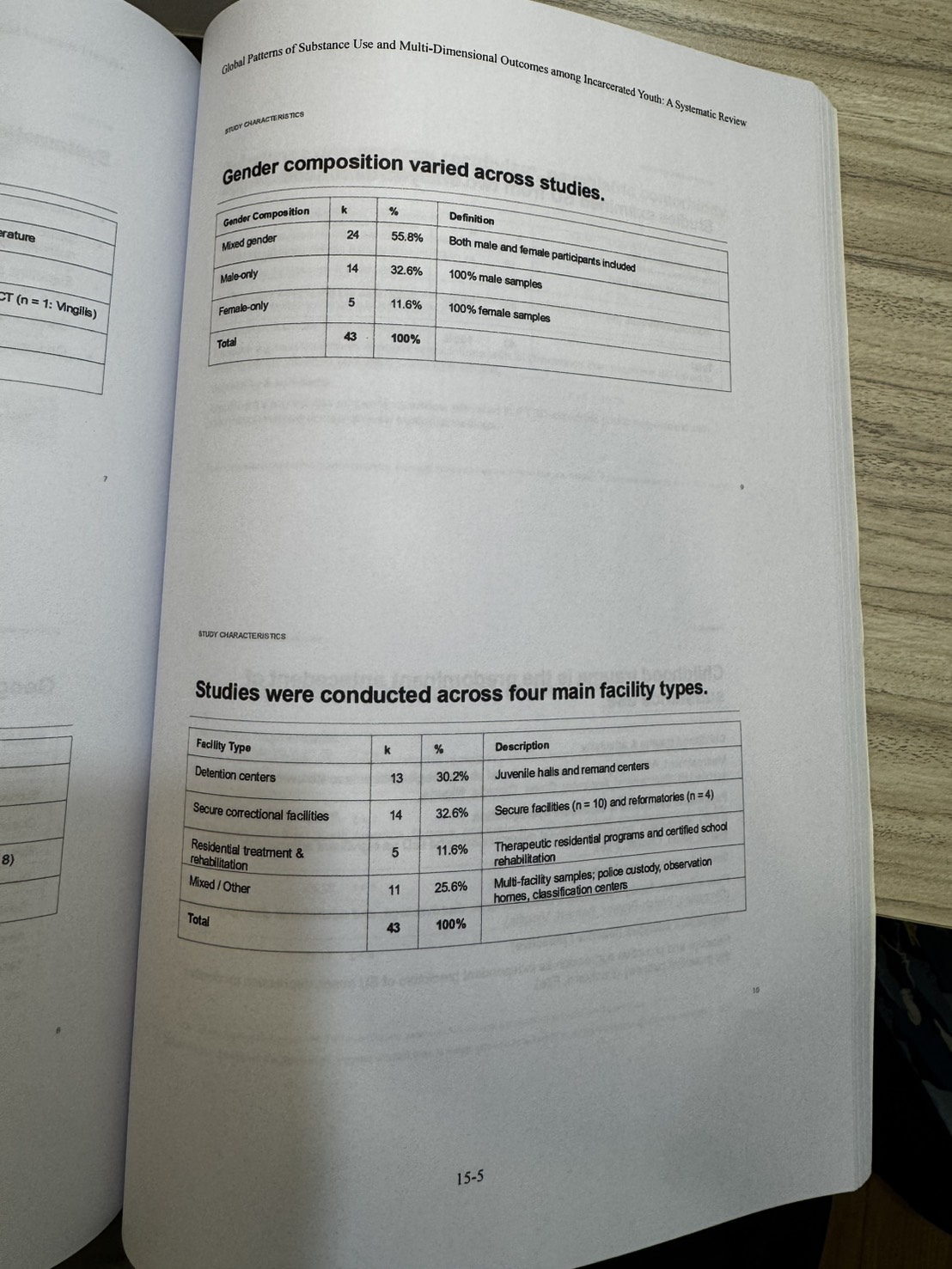
- 台灣可填補 Global South 的研究空缺——本研究 17 國中東亞僅佔 11.6%(中、日、韓),台灣的本土實證研究有國際發聲的迫切性。可與下午第 8、9 場(許華孚/葉碧翠)的本土實證資料連結至國際期刊。
- 對國教盟與兒少倡議聯盟的意涵:與本日上午第 4 場(國教盟主場「全人復元」)、下午第 7 場(中華民國兒童健康聯盟主場「少輔會結構」)形成三重證據鏈——個案、結構、國際——支持兒少倡議聯盟推動跨部會「創傷知情司法(trauma-informed justice)」立法。